False Localizing Signs, an overview
False localizing signs, definition
In majority of patients, a particular neurological sign indicating pathology at a specific locus or pathway within the nervous system.
False localizing signs refer to neurological signs that reflect pathology distant from the expected anatomical locus which make challenges in traditional clinicoanatomical correlation.
False localizing neurological signs have presented significant challenges to clinical neurologists.
Awareness of the possibility of false localizing signs, and knowledge of the situations in which they are most likely to occur, is necessary.
False localizing signs may be indicative of serious, even life threatening, pathology within neural pathways.
False localizing signs occur in two major contexts:
- Raised intracranial pressure
- Spinal cord lesions
False localizing signs due to intracranial lesions
Sixth nerve palsy
Sixth nerve palsy, either unilateral or bilateral, is the classic example of a false localizing sign.
The pathophysiological mechanism includes:
- stretching of the nerve in its long intracranial course
- Compression against the petrous ligament or the ridge of the petrous temporal bone
- backward brain stem displacement
Fifth and seventh nerve palsy
Has also been reported with raised intracranial pressure (e.g., Posterior fossa neoplasms or more diffuse neoplastic disease, and with IIH).
This dysfunction may be hypoactive or hyperactive, manifesting with negative or positive symptoms:
- Trigeminal neuropathy vs. Trigeminal neuralgia; sensory symptoms more predominant
- Facial palsy of LMN type vs. Hemifacial spasm
Most often occur at the same time as, or after, the development of sixth nerve palsies.
Trigeminal neuralgia and hemifacial spasm have only been reported in the context of posterior fossa mass lesions, most usually tumors.
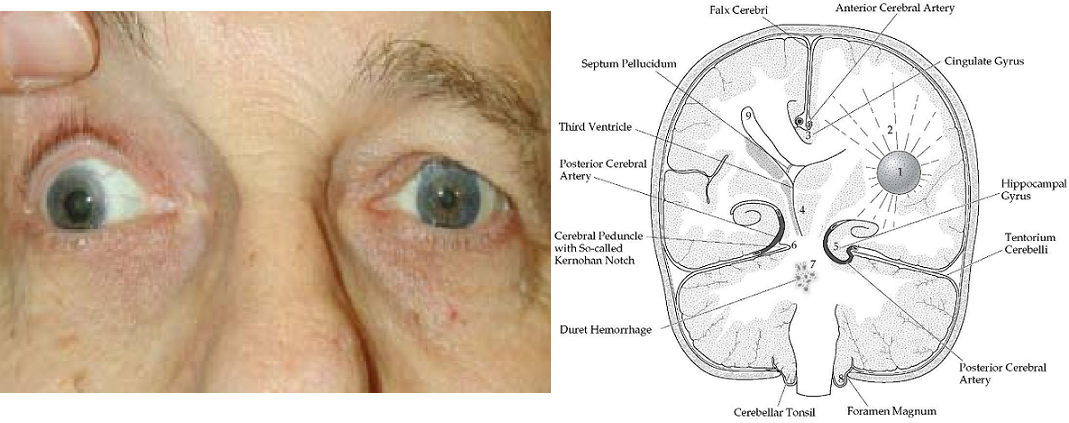
Third nerve palsy
Uncal herniation may be associated with third nerve palsy.
Unilateral mydriasis (“Hutchinson’s pupil”) may be the earliest sign.
Fixed dilated pupil is ipsilateral to a supratentorial mass but can contralateral 3rd nerve as a false localizing sign.
The possible causes: extrinsic compression of the third nerve on the margin of the tentorium or kinking of the nerve over the clivus.
Herniation of the temporal lobe through the tentorial notch may successively compress the third nerve and the ipsilateral cerebral peduncle resulting into ipsilateral 3rd nerve palsy and contralateral hemiparesis.
On occasion, herniation may be associated with a false localising ipsilateral hemiparesis, known as the Kernohan notch phenomenon in which the free edge of the tentorium compresses the contralateral crus cerebri.
Other “False localizing signs” with intracranial lesions
1. Trochlear nerve palsy has occasionally been described, it might be overlooked because the signs are subtle
2. Unilateral hearing loss has been reported in IIH, although tinnitus is the more common otological problem in this condition
3. Unilateral papilloedemamay be described as false localising when associated with contralateral visual loss and optic atrophy due to subfrontal or middle cranial fossa en plaque meningioma (Foster-Kennedy syndrome)
False localizing signs with spinal cord lesions
Foramen magnum and upper cervical cord
Lesions at the level of the foramen magnum may produce false localizing signs: paresthesia in the hands and lower motor neuron signs in the upper limbs.
Similarly, a syndrome of “numb and clumsy hands” has been described with midline cervical disc protrusions at the C3/C4 level; concurrent with numbness of fingertips and palms, there may be a tightening sensation at mid-thoracic level.
Cervical spinal cord lesions at or above the level of C4 in which finger and hand dysaesthesia with hand muscle atrophy preceded limb spasticity or gait disturbance have been reported.
Three pathophysiological mechanisms have been proposed: arterial blood supply compromise, venous compression and stasis, mechanical stress over the spinal cord.
Lower cervical and upper thoracic cord
Because of the anatomical decussation of spinothalamic tract fibers two or three segments above the level at which they enter the spinal cord from their respective dermatomes, sensory levels two or three segments distant from the level of cord pathology to be observed clinically.
More distant sensory and motor signs may be observed.
Compressive cervical myelopathy may produce a false localizing thoracic sensory level, sometimes called a mid thoracic girdle sensation, in addition to lower limb weakness and hyperreflexia.
Lumbar spinal disease may be simulated by more rostral pathology; for example, urinary retention, leg weakness, and lumbar sensory findings may be the presenting features of high thoracic cord compression (clinicoradiological discrepancy of as much as 11 segments).